Washington, D.C. (May 14, 2020) – The American Association of Suicidology (AAS) commends the US Senate in passing The National Suicide Prevention Designation Hotline Act. The bill, sponsored by Senators Cory Gardner and Tammy Baldwin, officially designates 988 as the unique, three-digit phone number for the National Suicide Prevention Lifeline and the Veterans Crisis Line. AAS has been working closely with other leading suicide prevention and mental health organizations, lawmakers in Congress, and the Federal Communications Commission, to help ensure the bill provides appropriate funding for crisis centers while improving access for those in need of emotional support.
“It has been phenomenal to watch the effort involved with making this legislation happen,” said AAS CEO, Colleen Creighton. “We especially want to thank Senators Gardner and Baldwin for their continued life-saving advocacy for this bill and suicide prevention. We now shift our focus to the House where we heartily encourage them to pass this legislation as well.”
“Crisis centers are excited to see the priority and recognized importance of the work that we have been doing for years to provide vital support to those in our communities that are struggling. Creating a 988 system for behavioral health support is certainly a development that speaks to the needs within our communities across our nation. With this passage of legislation, we have taken only the first steps toward this vision. The importance of funding for this system to be successful cannot be understated. Providing for infrastructure, legitimate compensation and care for the call takers in this system is of immense importance to making a 988 successful in terms of quality and sustainability. We look forward to the challenges that lie ahead as we come together as a national crisis community to build a system of care and support for our neighbors, community and nation.” – Cheri Skelding, VP of Clinical Operations, Rocky Mountain Crisis Partners (AAS Accredited Crisis Center)
In 2018 there were 48,344 suicide deaths in the US, with an age adjusted rate of 14.2 per 100,000 population. In the same year there were nearly 1.2 million suicide attempts.
For the Media: Responsible reporting on suicide, including stories of hope and resilience, can prevent more suicides. Please visit the Suicide Reporting Recommendations for more information.
About AAS: The American Association of Suicidology is the world’s largest membership-based suicide prevention organization. Founded in 1968 by Edwin S. Shneidman, PhD, AAS promotes the research of suicide and its prevention, public awareness programs, public education and training for professionals and volunteers. The membership of AAS includes mental health and public health professionals, researchers, suicide prevention and crisis intervention centers, school districts, crisis center volunteers, survivors of suicide loss, attempt survivors, and a variety of laypersons who have in interest in suicide prevention. You can learn more about AAS at www.suicidology.org.
ER Physician Shares Important Tips for Frontline Workers
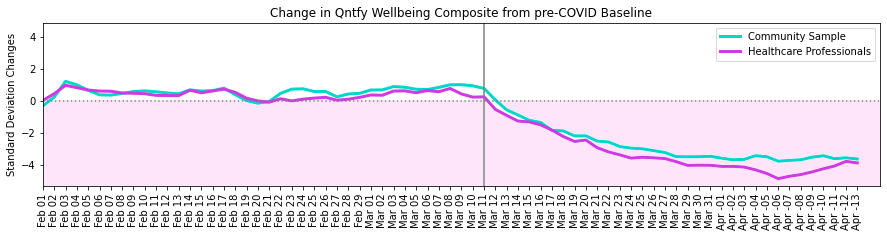
Washington, D.C. (May 5, 2020) – In cooperation with the American Association of Suicidology (AAS), Qntfy, an artificial intelligence analytics firm, launched a study looking at the effects of the pandemic on the mental well-being of the public compared to that of healthcare providers. Data on more than 25,000 healthcare professionals and more than 10,000 members of the general population were analyzed using machine learning models for anxiety, depression and suicide risk to develop Qntfy’s patented well-being scores. While the wellbeing of the general population has decreased, the wellbeing of the healthcare providers has decreased even more, which is cause for significant concern.
Qntfy uses its machine learning models to anonymously score social media messages posted by individuals in each category. These data were featured on NBC Nightly News on May 3, 2020.
Tony Wood, Qntfy Co-Founder shared: “These data may seem grim, but thankfully it contains a map of the path forward. Analytics like these can help the helpers, we can flatten the curve of the coming crisis in our behavioral healthcare system if we act now.”
The plot seen below is the average Qntfy well-being score per day for healthcare workers and the general population. Mental health, as it’s measured here, has decreased since the onset of COVID-19 and the associated lockdowns (indicated here by a vertical gray line around March 11th).
“We’re seeing an increasingly obvious toll of the COVID-19 pandemic on the mental health of frontline healthcare workers,” said Loice Swisher, an emergency room physician in Philadelphia and a member of the American Association of Suicidology. “Just like we need the appropriate supplies of personal protective equipment (PPE) for physical health/protections, we need the right kinds of mental health PPE. Like gloves, goggles, or masks, there are multiple different ways one can guard one’s mental health. And like with physical PPE, it is important to have it on and know how to use it before it becomes imminently necessary.”
Dr. Swisher recommends the first part of mental health PPE for all healthcare workers should involve developing a Personal Crisis Management Plan (PCMP). This is a version of a safety plan, which has been well established in suicide prevention crisis intervention services, but adapted with the needs of healthcare professionals in mind. There are also smartphone apps that include these features, like the Virtual Hope Box (Apple, Google).
Secondly, Dr. Swisher suggests healthcare workers who might find themselves at risk for a crisis to develop self-care strategies that focus on the following:
Connectedness – Maintain personal relationships. Identify three people you can call.
Calling or Purpose – Develop a “sunshine file” of great cases, thank you notes, pictures, or anything else that is important to you.
Compassion – Intentionally develop skills of mindfulness and self-compassion. Engage in curiosity, creativity, generosity, thankfulness, and wonder.
Finally, Dr. Swisher recommends these resources from the Council of Residency Directors in Emergency Medicine. Crisis Text Line has also established a program for frontline workers. More resources, as well as a tool to immediately find the closest crisis services can be found at covidmentalhealthsupport.org.
AAS is dedicated to continue working with its partners, members, and subject matter experts to respond to this changing crisis by providing life-saving resources with real outcomes.
For the Media: Responsible reporting on suicide, including stories of hope and resilience, can prevent more suicides. Please visit the Suicide Reporting Recommendations for more information.
About AAS: The American Association of Suicidology is the world’s largest membership-based suicide prevention organization. Founded in 1968 by Edwin S. Shneidman, PhD, AAS promotes the research of suicide and its prevention, public awareness programs, public education and training for professionals and volunteers. The membership of AAS includes mental health and public health professionals, researchers, suicide prevention and crisis intervention centers, school districts, crisis center volunteers, survivors of suicide loss, attempt survivors, and a variety of laypersons who have in interest in suicide prevention. You can learn more about AAS at www.suicidology.org.
About Qntfy: Qntfy is a Boston based AI analytics company. Founded in 2014, Qntfy is dedicated to the intersection of machine learning and behavioral science. As part of their mental health mission, they help university researchers collect and examine social and wearable data from participants who opt-in to the analysis through the OurDataHelps.org project. They also operate a streaming analytics platform called CAP that provides always-on access to insights (like the above) to enterprise, nonprofit, and government customers.
Washington, D.C. (May 1, 2020) – The American Association of Suicidology (AAS) was proud to host AAS20, its 53rd Annual Conference, as a complete and comprehensive virtual experience between April 23 – 25, 2020. Although AAS20 was on-track to be the best attended conference in the organization’s history, the organization canceled the in-person event due to health concerns related to the novel coronavirus pandemic and pivoted to an online event. Despite all this, more than 2800 people registered (1000 more than last year), making this the highest participation for an annual AAS conference, ever. This not only reflects the growing need for international suicide prevention initiatives, but also speaks to the quality of the conference content.
AAS felt a responsibility to uphold its role in providing the largest annual professional convening place for those who have been touched by suicide. Researchers, academicians, public health officials, prevention specialists and many more, were able to join online from across the world to establish effective strategies for addressing the rising suicide rate in this country. This year’s theme, Crossroads: Preventing Suicide and Creating Lives Worth Living, guided the programming, which was built on a framework of equity.
“We had a responsibility to our members and society at large to pivot online. It would have been hypocritical to plan a landmark conference – the first to look at suicidology through an equity lens – and then cancel during a time when people are dying because of long-standing inequities in health care, insurance coverage, and access to food and shelter,” said Jonathan Singer, PhD, President of AAS. “The fact that we were at record numbers for registration, sponsorship and exhibitions reflected the excitement that people were feeling around this theme. We had organized the most racially, ethnically and conceptually diverse group of invited speakers in the conference’s history. These speakers, along with the hundreds of presenters, were perfectly positioned to address equity and suicide prevention, intervention and postvention.
Even within a digital platform, AAS was able to provide one of the most inclusive and diverse lineups ever, with over 100 concurrent sessions and more than 25 speakers and subject matter experts were featured during our plenary and keynote sessions. The members of AAS wholeheartedly embraced the platform, engaging with presenters and content in new and exciting ways with the help of features like Chat and Live Q&A.
“We worked hard to make sure this year’s program focused on inclusivity, equity and giving a voice to those who often get overshadowed or forgotten by this field,” said Colleen Creighton, AAS CEO. “It was imperative that we did everything possible to continue with our conference; we owed it to our members. It was then both heartening and exciting to see our members support the pivot and embrace the virtual format in such a way that we exceeded all expectations and see the largest turnout for any of our conferences in our association’s 50+ year history”.
AAS also announced it will be providing a follow-up AAS20 Academy, which will provide access to all the recorded sessions from throughout the conference to everyone in attendance and anyone who registers post-conference. This will allow unprecedented access to breakout sessions not previously possible with in-person conference experiences. The organization will use this platform to continue adding content from speakers and experts through the Summer and Fall of 2020.
In 2018 there were 48,344 suicide deaths in the US, an age adjusted rate of 14.2 per 100,000 population. In the same year there were nearly 1.2 million suicide attempts.
For the Media: Responsible reporting on suicide, including stories of hope and resilience, can prevent more suicides. Please visit the Suicide Reporting Recommendations for more information.
About AAS: The American Association of Suicidology is the world’s largest membership-based suicide prevention organization. Founded in 1968 by Edwin S. Shneidman, PhD, AAS promotes the research of suicide and its prevention, public awareness programs, public education and training for professionals and volunteers. The membership of AAS includes mental health and public health professionals, researchers, suicide prevention and crisis intervention centers, school districts, crisis center volunteers, survivors of suicide loss, attempt survivors, and a variety of laypersons who have in interest in suicide prevention. You can learn more about AAS at www.suicidology.org.
###
Mental health providers & digital health solutions offer resources to encourage timely access to mental health crisis services
WASHINGTON, D.C., April 28, 2020 – According to the National Alliance on Mental Health, almost 1 in 5 Americans experience mental health concerns each year, while more than 100 die by suicide every day. COVID-19 crisis precautions introduced such as social distancing and self-isolation, coupled with the fear of medical emergencies and growing anxiety about the prolonged nature of the crisis, could amplify the number of people suffering from mental health concerns across the US. With Qualtrics reporting that 41.6% of the population has seen a decrease in their mental wellness since the COVID-19 outbreak, an innovative website resource aims to help alleviate their suffering.
As COVID-19 emergencies consume precious healthcare resources, timely access to mental health crisis care has never been more critical. With 20,000 – 40,000 people being admitted to emergency departments across the US each day for psychological purposes, providing a pathway to crisis care is essential. Across the world, a coalition of digital health solutions companies and mental health crisis responders called the Pandemic Crisis Services Response Coalition have designed a website to make it easier for Americans to prevent a mental health crisis while accessing available treatment when it is necessary.
The website, www.covidmentalhealthsupport.org, includes three main sections: guidance for people in crisis wishing to access support, guidance for helping a loved one in crisis, and resources for health care professionals.
“The ability to access mental health crisis services is critical at this time, yet COVID-19 is impacting the typical ways people receive help in a crisis,” says Travis Atkinson, president of the Crisis Residential Association and co-chair of the American Association of Suicidology’s Crisis Services Committee. ”As Emergency Rooms focus their capacity on COVID-19 patients, and psychiatric hospitals decrease their census to conform to social distancing guidelines, people in crisis need to know how to access available mental health services.”
Digital health solutions partners including KeepAppy, Live For Tomorrow, and All Mental Health are contributing to the cause.
“It has never been more important to take preventative action for mental health than now, in the face of the mental illness crisis coming as a result of COVID-19,” says Aimée-Louise Carton, co-founder of KeepAppy. “Using digital health and WellTech solutions will be a key mechanism for creating a bridge of preventative mental wellbeing support during this time of social distancing and isolation.”
While there is suffering as a result of COVID-19 that is unavoidable, mental health suffering can be prevented or minimized with the right interventions. The Pandemic Crisis Response Services Coalition is committed to doing all that we can to prevent additional deaths of despair due to consequences of our current situation..
The Pandemic Crisis Services Response Coalition members:
All Mental Health
American Association of Suicidology
Centerstone
CONTACT-USA
Crisis Residential Association
Crisis Text Line
Headstream
KeepAppy
Live For Tomorrow
National Action Alliance for Suicide Prevention
National Association of Crisis Organization Directors
RI International
National Suicide Prevention Lifeline
SilverCloud
TBD Solutions
The Trevor Project
KENTWOOD, MI (April 10, 2020): A recent national survey of behavioral health crisis service providers reveals that crisis services are severely impacted by the effects of COVID-19, as workers are overwhelmed and service demand is fluctuating dramatically. This includes Mobile Crisis Teams, Crisis Residential Programs, and Crisis Call Centers across the country.
A report released by TBD Solutions LLC in conjunction with other leading mental health
organizations analyzed the responses of over 350 crisis providers, including 147 Mobile Crisis
Teams, 130 Crisis Residential Programs, and 93 Crisis Call Centers. The research revealed a
crisis system susceptible to the same issues as its medical counterparts that must be treated
with the same heightened consideration. Survey responses were elicited from members of the
American Association of Suicidology, the Crisis Residential Association, and the National
Association of Crisis Organization Directors.
“As illness spreads in our area, there will be reduction in our workforce due to illness, isolation,
and return-to-work policies,” one respondent to the survey stated. “Staff [have] concerns about
continuing to work amid the public health concern.”
“The longer COVID-19 progresses in the United States, the greater the importance of behavioral
health crisis services on public health,” says Travis Atkinson, Crisis Systems Consultant with
TBD Solutions. “This pandemic has become the great equalizer for helpers and persons served,
yet the physical and mental stability of our behavioral health workforce is crucial in preventing
and treating mental health crises and avoiding the unintended consequences of social
distancing, such as suicide and untreated mental illness.”
Responses to the survey fell into six main categories:
Staffing: Morale and workforce stability have been compromised, leaving supervisors with few solutions to keep their services intact.
Health Concerns: Employees maintain a fear of contracting and/or spreading COVID- 19.
Clinical Services and Client/Caller Support: With so much attention and energy devoted to COVID-19 risks, programs have less human and financial resources to devote to treatment interventions.
Equipment/Supplies/Technology: Dozens of respondents reported inadequate supplies of critical PPE needed to do their jobs, and limited technology and IT equipment is inhibiting some Crisis Call Centers and Mobile Crisis Teams from moving to a remote workforce.
Operations/Sustainability: When some crisis services exist in fee-for-service models, reduced referrals means reduced income, forcing some providers to make difficult staffing and operations decisions.
Community Resources: Outpatient therapists, homeless shelters, psychiatric hospital beds, primary care clinics, and other critical resources have reduced service capacity or offer services remotely, an option that is not accessible for those with limited resources. “Crisis services play such an absolutely vital role in ensuring our nation’s health and well-being,” says Colleen Creighton, CEO of the American Association of Suicidology. “Unfortunately, this study illuminates just what an incredible burden COVID-19 is placing on an already underfunded, at near-capacity system. These are individuals that continuously sacrifice their time to selflessly care for us and our communities, day-in and day-out, all year round. As the national conversation turns to our country’s recovery, we need to work to ensure that behavioral health crisis services and their needs are a factor in that dialogue.”
MOBILE CRISIS CHALLENGES: Mobile Crisis Teams reported an overwhelmed workforce due
to health concerns (71%) and a lack of critical supplies (71%), such as Personal Protective
Equipment (PPE). More than 1 in 3 teams reported inadequate technology to work remotely
(37%), increased demands on first responders with care coordination (36%), and an
overwhelmed workforce due to fewer staff.
Forty-eight percent of Mobile Crisis Teams reported a decrease in calls.
CRISIS RESIDENTIAL CHALLENGES: 70% of Crisis Residential Programs reported an
overwhelmed workforce due to health concerns and a lack of critical supplies as major
concerns. Over half of respondents also cited attrition due to health concerns (53%) and an
overwhelmed workforce due to fewer staff (51%) as considerable challenges.
Forty-eight percent of Crisis Residential Programs reported a decrease in referrals.
CRISIS CALL CENTER CHALLENGES: Crisis Call Centers identified lack of critical supplies
(47%), an overwhelmed workforce due to increased referrals (45%), and attrition due to health
concerns (35%) as their most pressing challenges.
Almost half (49%) of all respondents reported an increase in call volume since the onset of COVID-19, with some stating they are receiving double the usual volume.
About TBD Solutions LLC: TBD Solutions (Kentwood, Michigan) is a national consulting, training, and research firm specializing in behavioral health crisis system design, function, and performance. Formed in 2011, TBD Solutions is committed to the values of high-quality, cost- effective, and client-centered care that effectively meets the urgent and ongoing needs of individuals receiving services. Learn more at www.tbdsolutions.com.
About AAS: The American Association of Suicidology is the world’s largest membership-based suicide prevention organization. Founded in 1968 by Edwin S. Shneidman, PhD, AAS promotes the research of suicide and its prevention, public awareness programs, public education and training for professionals and volunteers. The membership of AAS includes mental health and public health professionals, researchers, suicide prevention and crisis intervention centers, school districts, crisis center volunteers, survivors of suicide loss, attempt survivors, and a variety of laypersons who have in interest in suicide prevention. You can learn more about AAS at www.suicidology.org.
About CRA: The Crisis Residential Association and its members exist to support the operational and clinical functions of residential alternatives to psychiatric hospitalization. Rooted in the values of empathy, recovery, and continuous improvement, the association seeks to connect providers with the best ideas in behavioral health treatment to transform the way people receive mental health care. More information is available at www.crisisresidentialnetwork.com.
About NASCOD: The National Association of Crisis Organization Directors is an organization for social service professionals serving as Executive Directors or Program Directors of crisis organizations. NASCOD’s mission is to provide support and professional development for executive directors and program managers. More information is available at www.nascod.org.
Washington, D.C. (February 26, 2019): The American Association of Suicidology (AAS) is pleased to announce that Keita Franklin, LCSW, PhD, Chief Clinical Officer for Psych Hub, has joined its Board of Directors. With over 25 years of progressively responsible experience, Dr. Franklin has spent her career driving complex organizational change in the federal sector, improving the systems that provide care for our Nation’s military, family members, and veteran populations.
“I am thrilled about joining the AAS Board of Directors!” said Dr. Franklin. “After close to two decades in federal service where I have worked on multiple task forces and coalitions across various sectors, I am excited about transferring these skills to the non-profit arena to help advance the goals of AAS. I have a keen interest in continuing to advance the national dialogue and implementation of programs surrounding military, family member, and veteran suicide prevention issues. I look forward to contributing and working alongside the dedicated AAS team and fellow board members on important areas like strategic planning and advancement of training initiatives that help to save lives.”
In her current role as Chief Clinical Officer for Psych Hub, she serves as a key member of the executive team overseeing the development and production of all clinical content for Psych Hub’s learning platform of educational training courses and support tools on evidence based practices. A nationally-recognized expert, Dr. Franklin, ensures all clinical content is evidence based and focused on a practical application of the science.
“We’re ecstatic to have Dr. Keita Franklin join the Board,” said Colleen Creighton, CEO of AAS. “Her connection to military and veterans issues will help focus our efforts in these areas and sharpen our effectiveness in helping these groups. Her extensive background in training development and implementation will also be invaluable as we look to enhance our world-class training and accreditation programs.”
Before joining Psych Hub, Dr. Franklin served as a senior executive at both the Department of Veteran Affairs and the Department of Defense. In these roles, Dr. Franklin served as the principal advisor to Department leadership for all matters on suicide prevention, and she is widely credited with leading a transformative, enterprise-wide shift from a crisis intervention posture to an upstream, broad public policy approach focused on continuous surveillance and early prevention.
AAS is dedicated to providing representation that effectively communicates the needs and goals of its membership. By continuing to include a diverse roster of individuals who can address these components, AAS, its committees, and its Board of Directors work strategically to create programs focused on ending suicide in this country and throughout the world.
For the Media: Responsible reporting on suicide, including stories of hope and resilience, can prevent more suicides. Please visit the Suicide Reporting Recommendations for more information.
About AAS: Founded in 1968 by Edwin S. Shneidman, PhD, AAS promotes the research of suicide and its prevention, public awareness programs, public education and training for professionals and volunteers. The membership of AAS includes mental health and public health professionals, researchers, suicide prevention and crisis intervention centers, school districts, crisis center volunteers, survivors of suicide loss, attempt survivors, and a variety of lay persons who have in interest in suicide prevention. You can learn more about AAS at www.suicidology.org.
Washington, D.C. (February 25, 2020) – The American Association of Suicidology (AAS) is proud to host AAS20, its 53rd Annual Conference, in Portland, OR at the Marriott Downtown Waterfront hotel, April 22 – 25, 2020. Thousands will be in attendance this year, once again making it the largest professional convening place for those who have been touched by suicide. Researchers, academicians, public health officials, prevention specialists and many more, will all join to establish effective strategies for addressing the rising suicide rate in this country. This year’s theme, Crossroads: Preventing Suicide and Creating Lives Worth Living, guided the programming, which was built on a framework of equity.
“AAS has made it a priority to center the voices of black, indigenous, and people of color, not only during the presentations at AAS20, but throughout the development of the program for years to come,” said Dr. Jonathan Singer, President of AAS. “For the field of suicidology to truly begin to make a difference, not just in terms of rates of suicide, but regarding ethical considerations of treatment and prevention, we must first acknowledge the long-standing inequity of services and resources in this country.”
In one of our most inclusive and diverse lineups ever, speakers and subject matter experts featured during our plenary and keynote sessions will address how equity has (and has not) played a role in the prevention, intervention, and postvention of suicide in the US, both historically and currently. The Press Kit highlights this incredible array of speakers.
“We’re welcoming key leading voices with backgrounds in science, research, lived experience, and those with clinical expertise, to start breaking down these barriers between disciplines and to strike at the heart of suicide,” said Colleen Creighton, AAS CEO. “By clearing the way for real conversations to happen, for real work to be done, we can be more effective in understanding the causes behind suicide. Those conversations, that work, all begins here at AAS.”
We have an opportunity to be open to new ideas, new approaches, and to engage with unfamiliar scientific, cultural, and community-based approaches examining and highlighting suicide prevention in ways we never would have imagined. In order to move forward in a way that is inclusive and centers diverse experiences, it is necessary to explore some of the tensions underlying our field. Disparities exist in suicide prevention, not just in rates of suicidal thoughts and behaviors, but in leadership, representation, research, funding, and in the data we prioritize. In order to prioritize equity, we must intentionally re-dedicate ourselves to doing this work with equity and inclusivity.
At AAS20, we will sharpen our focus and highlight new voices. Specifically, we will honor those transformed by suicide, present innovative research and intervention practices, while integrating social trends to chart new, cohesive and efficient paths to reduce suicide and create a world worth living in. This is our opportunity to make lasting changes to our field and we look forward to you joining us.
In 2018 there were 48,344 suicide deaths in the US, an age adjusted rate of 14.2 per 100,000 population. In the same year there were nearly 1.2 million suicide attempts.
For the Media: Responsible reporting on suicide, including stories of hope and resilience, can prevent more suicides. Please visit the Suicide Reporting Recommendations for more information.
About AAS: The American Association of Suicidology is the world’s largest membership-based suicide prevention organization. Founded in 1968 by Edwin S. Shneidman, PhD, AAS promotes the research of suicide and its prevention, public awareness programs, public education and training for professionals and volunteers. The membership of AAS includes mental health and public health professionals, researchers, suicide prevention and crisis intervention centers, school districts, crisis center volunteers, survivors of suicide loss, attempt survivors, and a variety of laypersons who have in interest in suicide prevention. You can learn more about AAS at www.suicidology.org.
BOSTON – (February 18, 2020) – Physician and nurse leader burnout is a public health crisis that demands action across the entire healthcare ecosystem. Burnout not only affects clinicians, but also the entire health system and the patients who depend on quality medical care. At the first annual Physician Burnout Symposium, we will gather thought leaders and stakeholders for a two-day conference to address the many facets of burnout, such as time constraints, technology and regulations. Attendees will gain actionable solutions to implement in their health systems.
The Patient Experience Symposium is partnering with the Sharp Index, a nonprofit dedicated to improving physician well-being and ending physician suicide, to share different voices about how to address and reduce burnout and restore joy in practicing medicine. In addition to the symposium, the Sharp Index will host an annual awards reception on June 23, 2020 at the same venue.
“When our physicians struggle, we all lose. We can’t have good health without them,” said Janae Sharp, founder of the Sharp Index and a suicide loss survivor. “It’s critical that our leaders come together to identify and implement the solutions to the physician burnout crisis. This conference will help them do exactly that.”
A critical topic covered at the conference is clinician suicide, and we are very happy to have the American Association of Suicidology (AAS) partnering with us for our inaugural event. The AAS promotes the research of suicide and its prevention, public awareness programs, public education and training for professionals and volunteers.
“It’s critical to take care of those who take care of us,” said Colleen Creighton, CEO of AAS. “The demands and expectations of our physicians, medical students, those in residency and those reaching the end of their careers, have grown exponentially over the last few decades. We know there is a suicide crisis in the medical profession and having the conversations highlighted at this conference is an important way to save more lives.”
The Physician Burnout Symposium will consist of a half-day of pre-conference workshops focusing on technologies and innovations that help reduce burnout, enabling conference delegates to dive deeper before the main conference begins. Some expert speakers include:
Paul DeChant, MD, MBA, CEO/Principal of Paul DeChant, LLC
Ron Paulus, MD, President and CEO, RAPMD Strategic Advisors
Todd Dunn, Director of Innovation: Intermountain Healthcare Transformation Lab at Intermountain Health
Dese’Rae L. Stage, Artist, Mom, Suicidologist, Activist
Elisa Arespacochaga, VP, Physician Alliance, American Hospital Association
Vivek Garg MD, Chief Medical Officer, CareMore Health
Kevin D. Hopkins, MD, Primary Care Medical Director, Cleveland Clinic
J. Bryan Sexton, MD, Associate Professor in Psychiatry and Behavioral Sciences, Duke University School of Medicine
Jonathan B. Singer, Ph.D., LCSW, President, American Association of Suicidology
“We are very excited to be working with The Sharp Index and American Association of Suicidology on this important topic to help reducing clinician burnout while enhancing healthcare organizations’ performance and viability.”, stated Conference Director and President of ICDevents, Bill Doherty.
International Conference Development, LLC (ICDevents) produces high-quality conferences and tradeshows in a broad range of industries. Utilizing intensive, detailed market research, ICDevents creates targeted events designed to encourage companies to send their entire teams to problem-solve, network, and brainstorm with other industry leaders, consultants, and suppliers.
About Sharp Index:
The Sharp Index is a nonprofit dedicated to reducing physician suicide through awareness, best practices, and data science. We advocate for the use of human-focused and data-backed solutions to achieve greater physician well-being and stronger patient care. Together we can create a system to heal the healers. We are interested in conversations that bring more attention to solutions that improve physician well being and empower each individual to make a difference. We also look at system change and raise awareness about improving this complex problem. You can learn more about the Sharp Index at www.sharpindex.org.
About American Association of Suicidology (AAS):
Founded in 1968 by Edwin S. Shneidman, PhD, AAS promotes the research of suicide and its prevention, public awareness programs, public education and training for professionals and volunteers. The membership of AAS includes mental health and public health professionals, researchers, suicide prevention and crisis intervention centers, school districts, crisis center volunteers, survivors of suicide loss, attempt survivors, and a variety of lay persons who have in interest in suicide prevention. You can learn more about AAS at www.suicidology.org.
The American Association of Suicidology (AAS) appreciates the opportunity to submit comments and express our support for the Federal Communications Commission’s (FCC) proposed rule, Implementation of the National Suicide Hotline Improvement Act of 2018. AAS is the nation’s oldest and largest membership-based suicide prevention organization. Founded in 1968, our mission is to promote the understanding and prevention of suicide and to support those who have been affected by it.
Suicide is a massive public health issue in this country. Equitable access to appropriate care, is critical and necessary to ensure people receive the services they require in their time of need or crisis. Additionally, by providing access to rapid care, as in telephonic or texting resources, other services are less likely to be overwhelmed or strained. For instance, the ability for more suicidal crises to be diverted away from emergency services has the potential to alleviate costs to hospital systems and municipalities.
AAS fully supports the FCC’s proposed rule plan to identify a three-digit number – 9-8-8 – to be designated for suicide and other mental health crises. It is also absolutely necessary that these changes are made in ways that limit the amount of potential confusion regarding the transition from the previous number. AAS supports the use of a media campaign to highlight the change with a “launch” date to better distinguish the turn-on of the service, followed by sustained messaging after the fact. Messaging and service provision should include distinct programs for different high-risk populations, such as LGBTQA+, Native American/Alaskan Native, Military Service Members, and others.
AAS also fully supports the use of contemporary technologies as part of these suicide and mental health crises responses, not only telephonic services. In the last 6 years, Crisis Text Line has handled 129 million messages, accomplished over 50,000 crisis de-escalations, and initiated over 30,000 active rescues (interactions where emergency services were required). The ubiquitous use of text messaging, especially among our youth, will require this modality to be included in the processes outlined by the FCC.
Furthermore, the critical nature of these services requires that crisis centers answering calls and texts from those in crisis be adequately resourced to handle the inevitable increase in volumes of contacts. Many crisis centers are underfunded and understaffed. To ensure that crisis calls are answered locally and in a timely fashion, these centers need the appropriate resources to operate at levels that meet the scale of the demand. The legislation implementing the FCC’s plan must include a funding mechanism that ensures crisis center sustainability and enhanced capacity. It is vital that participating centers meet nationally recognized crisis standards by accrediting bodies and implement the evidence-based practices championed by the National Suicide Prevention Lifeline.
As an organizational leader in the field, AAS believes that establishing a unique, 3-digit number for mental health and suicide prevention offers a unique opportunity increase the effectiveness of crisis services in this country. Thank you for your leadership as we work to improve the lives of Americans.
Washington, D.C. (January 30, 2020) – The CDC’s most recent suicide-related data in its annual mortality and life expectancy report once again highlights the public health crisis of suicide in this country. This report indicates that there were 48,344 suicide deaths in the US in 2018 and the rate increased from 14 per 100,000 population in 2017 to 14.2 per 100,000 population in 2018. Previous reports have shown increases in suicide deaths among all demographic groups as well, further illuminating the critical need to fund comprehensive suicide prevention initiatives in the US.
“As the rate of suicide continues to climb in this country, year over year, it is necessary to focus on the few effective suicide prevention strategies we’re aware of,” said Jonathan Singer, President of the American Association of Suicidology (AAS). “We’re at a tipping point, where we understand some fundamental, effective prevention methods, but must develop population-level implementation. This includes the potential of implementing non-traditional, alternative methods of intervention like community-based strategies that expand the scope of suicide prevention beyond mental health responses.”
There is only speculation as to why suicide rates are rising in the US. It remains important for the media, suicide prevention, and mental health organizations to communicate to the public that any single explanation for why individuals attempt or die by suicide is insufficient. In fact, it could be detrimental to imply that we can explain its causes without direct scientific evidence to support such claims. Conversely, this means that no single approach to solving the problem of suicide is sufficient, but rather a multidisciplinary, multi-sector strategy is necessary.
Systems for gathering data about suicide deaths, attempts, and ongoing suicidal experiences are significantly underdeveloped and undersupported. The US must establish better epidemiology around suicide, as well as develop innovative methods for collecting data at scale so our best researchers can help us understand what is happening. This specifically includes funding for suicide prevention at the scale of the problem, nationally, regionally, and locally. If we continue to fund suicide prevention research in a piecemeal way, we will never understand its causes or effectively support its prevention at scale. Recent increases in funding for the CDC and NIH are an excellent start but do not reflect the size and scope of the public health crisis.
“Among the very few things we have evidence for showing an impact on suicide rates, like crisis lines, training of healthcare professionals, and maintained contact with people experiencing thoughts of suicide, access to lethal means is one of the most important for us to focus on,” said Colleen Creighton, CEO of AAS. “By putting space and time between someone experiencing thoughts of suicide and their method, namely firearms, we greatly increase their chances of survival. We see very promising research surrounding firearms safety legislation and its potential to reduce suicide rates at population levels.”
In the US, there is no national requirement for crisis response training among healthcare professionals despite suicide being the 10th leading cause of death. No national standard suicide risk assessment or standardized requirement for suicide care yet exists in the private healthcare system. It is left to individual health systems to make suicide-safer care a priority. Few regulatory bodies are currently invested in the research that would make such standards of care mandatory for every patient or client. Given the scope of the public health crisis of suicide, training and regulatory bodies have much room to improve the systems of care and ensure providers are ready to help someone at risk of suicide.
There is also increased attention being paid to suicide prevention in the form of new, bipartisan legislation for a three-digit, crisis intervention and mental health hotline. Congresspeople, the FCC, and many others in the telecommunications industry are diligently working on creating and fully funding this resource to increase access for those in need.
From April 22-25, 2020, AAS will convene its 53rd Annual Conference in Portland, OR at the Marriott Downtown Waterfront where we anticipate thousands of suicidologists, researchers, clinicians, advocates, those with lived experience of suicide loss and attempts, and many more to discuss the topics outlined in this press release. We know it will take all of these individuals to reverse the upward trend of suicide rates in the US. Suicide Prevention is Everyone’s Business.
For the Media: Responsible reporting on suicide, including stories of hope and resilience, can prevent more suicides. Please visit the Suicide Reporting Recommendations for more information.
About AAS: The American Association of Suicidology is the world’s largest membership-based suicide prevention organization. Founded in 1968 by Edwin S. Shneidman, PhD, AAS promotes the research of suicide and its prevention, public awareness programs, public education and training for professionals and volunteers. The membership of AAS includes mental health and public health professionals, researchers, suicide prevention and crisis intervention centers, school districts, crisis center volunteers, survivors of suicide loss, attempt survivors, and a variety of laypersons who have in interest in suicide prevention. You can learn more about AAS at www.suicidology.org.